

Updates and Commentary on the Latest in Cancer
By Dr. Ajaz Bulbul
FDA Breast implant advisory for lymphoma
The U.S. Food and Drug Administration (FDA) in an advisory letter reached out to physicians and patients regarding the risks involved with breast implant-associated lymphoma in women. Part of the FDA’s job is to provide up-to-date education and information on health trends and risk advisories. This provides patients and providers with valuable information to have a thorough and thoughtful discussion weighing the benefits and risks of different products.
FDA issued an update regarding the number of cases of breast implant-associated anaplastic large cell lymphoma (BIA-ALCL), a type of non-Hodgkin’s lymphoma and a known risk from breast implants. In 2011, the FDA was the first public health agency in the world to communicate about the risks of BIA-ALCL, warning women that the available information at the time indicated that there is a risk for women with breast implants for developing this disease.
As of September 2018, the agency has received a total of 660 total medical device reports regarding BIA-ALCL cases since 2010. Of the 660 MDRs, there are 457 unique cases of BIA-ALCL, including 9 patient deaths. There is an increase of 246 new MDRs since last year. The increased number of MDRs contributes to our evolving understanding of BIA-ALCL and represents a more thorough and comprehensive analysis.
A Patient Registry and Outcomes for Breast Implants and Anaplastic Large Cell Lymphoma Etiology and Epidemiology (PROFILE- registry), collects real-world data regarding patients who have a confirmed diagnosis of BIA-ALCL. FDA participates in the registry and this helps provide a Medical Device Safety Action Plan.
Both physicians and patients are also encouraged to file medical device reports with the FDA via MedWatch, the FDA Safety Information and Adverse Event Reporting program.
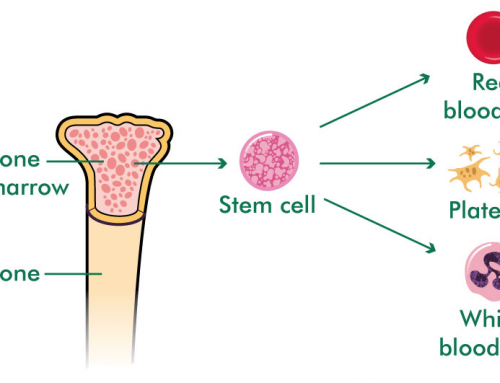
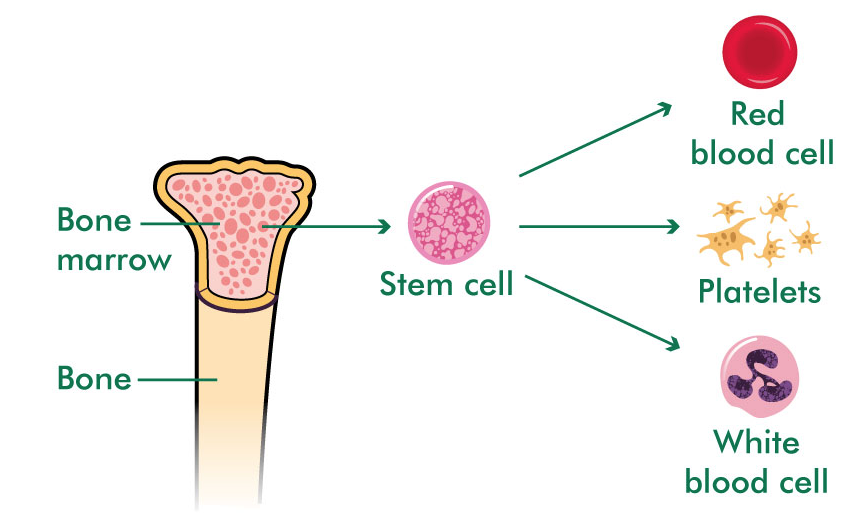
New drug in the pipeline for Refractory anemia or Myelodysplasia of the Bone marrow
A randomized, double-blind, phase III trial called the MEDALIST trial shows some exciting findings for patients of a pre-leukemia condition called MDS or myelodysplastic syndrome also called refractory anemia. This drug called luspatercept significantly reduced the need for frequent red blood cell transfusions in patients with lower-risk myelodysplastic syndromes (MDS), especially those with cells called ‘ring sideroblasts’ in the bone marrow. With luspatercept, about 38% remained transfusion-free for 8 weeks or longer, compared with 13% treated with placebo (sugar pill).
These responses were durable and long lasting with luspatercept. Approximately 40% of patients achieving red blood cell transfusion independence sustained after 12 months of treatment which is quite impressive.
For most of these patients, over time, the disease becomes blood transfusion-dependent. With that the complications of iron loading and chronic fatigue.
Luspatercept is an investigational first-in-class drug that neutralizes inflammatory proteins in the bone marrow called transforming growth factor-ß (TGF- ß). Inhibiting this bad signal enhances late-stage red cell maturation and increased cell population.
This study was conducted in about 65-centers including 229 patients internationally, with patients requiring ≥ 2 units of red blood cells every 2 months. All patients had either failed to respond to so-called growth factors that these patients have to receive typically weekly. This drug is given subcutaneously every 3 weeks for at least 6 months.
Last year’s rare cancer advances
Cancer treatment is progressing at a rapid rate, some would say some cancers are faring better than others. Usually, the more common the cancer is the more research dollars and focus on it means a faster pace of improvements. Progress is moving at a quicker pace than ever before now for much rarer cancers that have lacked research support. With new advances in immunotherapy and targeted therapies to new molecular diagnostics and the effect of the gut microbiome in impacting outcomes in cancer patients.
This year’s Clinical Cancer Advances from the American Society for Clinical Oncology, ASCO (the largest cancer organization) reported highlights the past year and the upcoming areas of promise.
Some of the important rare cancer advances, recognized by ASCO were:
- Anaplastic thyroid carcinoma: The U.S. (FDA) approved the first treatment for this type of thyroid cancer in nearly 50 years: a targeted-therapy combination of an oral drug called dabrafenib plus trametinib for patients with BRAF-mutated anaplastic thyroid carcinoma.
- Desmoid tumors: Research identified oral targeted drug commonly used in kidney cancer called sorafenib as the first therapy to improve progression-free survival for patients with this rare form of sarcoma.
- Neuroendocrine Tumors: The FDA approved 177 Lu-Dotatate, which delivers targeted radiation to tumor cells, lowering the risk of disease progression and death by 79%. This is a relatively common but malignancy with relatively long survival with newer treatments. We are quite excited about this drug.
- Uterus serous carcinoma: A breast cancer drug trastuzumab slowed the progression of HER2-positive uterine serous carcinoma, one of the most aggressive forms of endometrial cancer.
- Tenosynovial giant cell tumor: A novel drug Pexidartinib was shown to be the first promising therapy for this rare cancer of the joints.
New treatment for colon cancer
After some wait, exciting results of a clinical trial called BEACON trial are out. The triplet (three drugs) therapy that blocks three different pathways in colon cancer tumor cells in colon cancer tumors that express a signal marker called BRAF; also called BRAF-mutated colorectal cancer, a malignancy that typically does not respond to chemotherapy combination or even previous attempts to target BRAF mutation. Early results from the BEACON study showed an impressive 48% response rate and tumors did not progress for about 8 months on average which is at least 2 months more than a usual median progression-free survival of 6 months in second-line treatment.
BRAF mutations are detected in 10% to 15% of metastatic colorectal cancer. The phase III portion of the study is currently enrolling 615 patients to one of three arms. Patients will be treated until disease progression. This regimen is reasonably well tolerated. No serious signals were noted in this study
Reader Q&A
Q: I have thick blood, my primary care doctor said to cut down on smoking, what else should I do?
A: Thick blood would be a colloquium for something we call Polycythemia or high Red cell production. In other words, your body is producing too many blood cells.
The gist of your treatment would involve plenty of hydration, Aspirin (as long as you are not allergic to it or have peptic ulcer issues) and sometimes phlebotomy or blood donation is recommended so as to not allow your hemoglobin rise above safe levels that may lead to blood clots, leg cramps, MI, headaches, and even visual problems. The cause can be anything from sleep apnea, smoking, or a blood disorder.
You should see a Hematologist of a Blood specialist. I hope that helps.
Q: Dr. My doctor said I have low platelets. Do I risk bleeding spontaneously?
A: Low platelets is quite common if you tell me. As a Hematologist, I see it quite commonly. There are as many causes of it as there are episodes of Grey’s Anatomy (a lot!).
One diagnosis that is on top of our list is something called ITP or immune thrombocytopenia purpura. In simple parlance an immune system disorder where you white cells fail to recognize your own platelets and try to damage them. This is usually responsive to steroid use. It can be a refractory condition and requires a specialist who manages blood disorders. Other common causes could be drugs, infections, and rarely H pylori infection. Alcohol abuse and liver disease related to that or hepatitis C are also very common causes of low platelets. Extremely low numbers like less than 10 thousand platelets can lead to spontaneous bleeding. A normal platelet count is anywhere between 150 thousand to 400 thousand per decilitre of blood.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}